
A preprint report utilizing a New York state database of children ages 5-17 analyzed the effectiveness of the Pfizer-BioNTech COVID-19 jab.
The researchers estimated the mRNA injection’s efficacy against COVID cases and hospitalizations for the age demographics during December, 2021 and January, 2022.
The Abstract states:
In the Omicron era, the effectiveness against cases of BNT162b2 declined rapidly for children, particularly those 5-11 years.
Trending: Check Out My New Site, NoahReport!
Several weeks after becoming “fully vaccinated,” the efficacy of the Pfizer COVID-19 jab significantly waned for children.
For 5-11-year olds, the mRNA jab crossed a threshold of “negative” vaccine efficacy five weeks after “full vaccination.”
And by the sixth week, inoculated 5-11-year olds were 40% MORE likely to contract COVID-19 than their unvaccinated peers.
URGENT: mRNA shots raise the risk of Covid infection in children under 12 https://t.co/66qhh8czsd
— richard fredericks (@rfreder929) March 1, 2022
Alex Berenson explains in Unreported Truths:
The mRNA jabs provide some protection for the first two weeks of “full vaccination.” But it declines rapidly, turns negative by the fifth week, and more sharply negative in the sixth.
“Negative” vaccine efficacy means that vaccinated people are more likely to become infected. It is not clear how high the increased risk may become for young children, since the database only covered six weeks and the trend worsened each week.
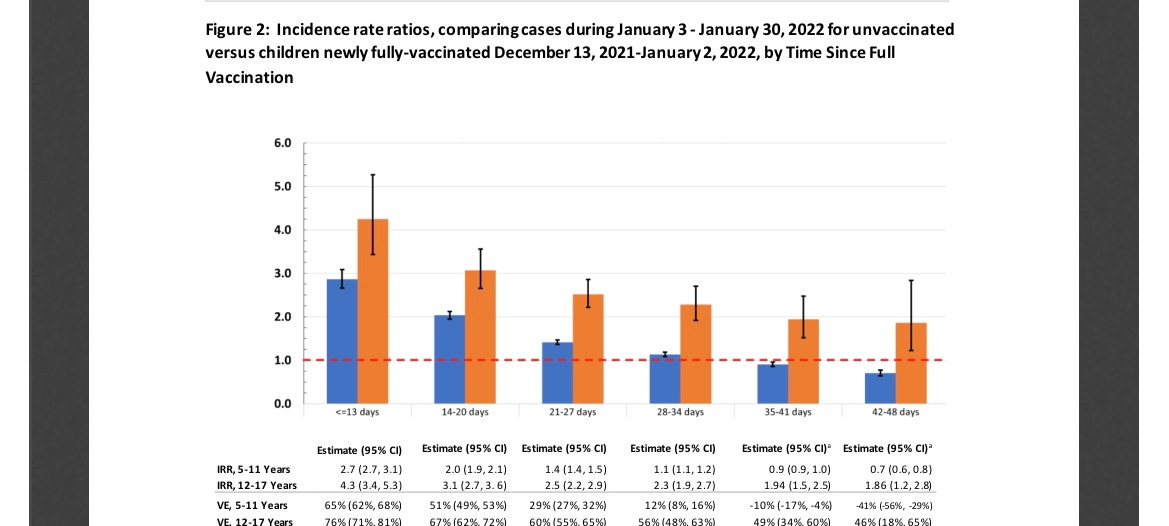
The blue bar in the chart below shows the relative odds of unvaccinated and vaccinated children to get Covid. The dashed red line equals a risk ratio of 1 – a 50/50 risk.
See how the blue bar falls each week and drops below the red line after 35 days? At point, unvaccinated children have lower risk. (The orange bar is kids 12-17. They still have some protection six weeks out, although it too is declining.)
The database included 365,000 inoculated 5-11-year olds in New York state.
Unsurprisingly, the researchers failed to mention the negative effectiveness in their discussion of their findings.
Here’s their discussion:
During Omicron variant predominance, VE against infection declined rapidly for NYS children 5-11 years, with low protection by one month following full-vaccination. Among children 12-17, protection declined substantially, albeit more slowly than observed among younger children. These results complement early findings of reduced primary series VE for ≥12 years during the Omicron era and the dual effects of the variant and waning protection against infection with sustained protection against severe disease.
The finding of markedly-lower VE against infection for children 11 years compared to those 12 and 13 years, despite overlapping physiology, suggests lower vaccine dose may explain lower 5-11 years VE. Children 12 years had the highest VE of all ages, potentially due to being small size relative to dose and more recent vaccination (by 6 weeks on average)than those 13-17 years. This gap suggests a threshold effect between the two BNT162b2 vaccine doses and need for study of numbers of doses, amount per dose, dose timing, and/or antigens targeted for children 5-11 years.
The findings in this study are subject to limitations. First, home testing, which is not reported and increased during the analysis period, would impact conclusions if testing practices differed by vaccine status. This potential bias would not impact hospitalizations. During this highest-incidence period, including for severe disease, for children, there were still relatively few children admissions. Additional data are needed to fully-understand VE trends against severe disease.2,9 By the end of January, 12.5% of vaccinated children 12-17 years had received a booster, likely adding protection to that group, although the time-since-vaccination analysis had no boosted children. This analysis compared early vaccinators in the younger age group with later vaccinators in the older age group, who may differ in test-seeking or exposures. Similar conclusions regarding relative VE declines between children 5-11 and 12-17 years using open cohorts suggests this trend is robust.
Our data support vaccine protection against severe disease among children 5-11 years, but suggest rapid loss of protection against infection, in the Omicron variant era. Should such findings be replicated in other settings, review of the dosing schedule for children 5-11 years appears prudent. At this time, efforts to increase primary vaccination coverage in this age group, which remains <25% nationally, should continue. Given rapid loss of protection against infections, these results highlight the continued importance of layered protections, including mask wearing, for children to prevent infection and transmission.
Join the conversation!
Please share your thoughts about this article below. We value your opinions, and would love to see you add to the discussion!